Overview
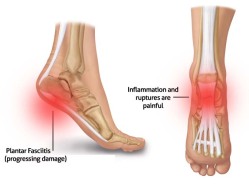
The plantar fascia is a thickened fibrous aponeurosis that originates from the medial tubercle of the calcaneus and runs forward to form the longitudinal foot arch. The function of the plantar fascia is to provide static support of the longitudinal arch and dynamic shock absorption. Individuals with pes planus (low arches or flat feet) or pes cavus (high arches) are at increased risk for developing plantar fasciitis.
Causes
Plantar fasciitis is caused by small, repetitive trauma to the plantar fascia. This trauma can be due to activity that puts extra stress on the foot. Plantar fasciitis is most common in people who are 40-60 years old. Other risk factors that increase your chance of getting plantar fasciitis include physical exertion, especially in sports such as running, Volleyball, tennis, a sudden increase in exercise intensity or duration, physical activity that stresses the plantar fascia. People who spend a lot of time standing, a sudden increase in activities that affect the feet, obesity or weight gain, pre-existing foot problems, including an abnormally tight Achilles tendon, flat feet, or an ankle that rolls inward too much. Poor footwear. Heel spurs.
Symptoms
Pain tends to start gradually, often just in the heel, but it can sometimes be felt along the whole of the plantar fascia. The symptoms are initially worse in the morning and mostly after, rather than during, activity. As the condition becomes worse, the symptoms become more persistent.
Diagnosis
A thorough subjective and objective examination from a physiotherapist is usually sufficient to diagnose plantar fasciitis. Occasionally, further investigations such as an X-ray, ultrasound or MRI may be required to assist with diagnosis and assess the severity of the condition.
Non Surgical Treatment
Cortisone is a powerful anti-inflammatory and when injected directly into the heel it will work almost immediately. Bear in mind however, that the treatment does not address the root cause of the inflammation, and needs to be repeated every few months. Also note, these injections are quite painful, and most doctors today will consider other, less invasive treatment options first. ESWT (Extra Corporeal Shockwave Treatment). A specialist targets therapeutic shockwaves to the affected heel area. This will stimulate a healing response in the affected tissue and ligaments, resulting in reduced inflammation and pain. This treatment and may take from 3 to 4 months to be fully effective. Extracorpreal Shock Wave Therapy is the latest technology to treat chronic plantar fasciitis. It is a non-invasive treatment and highly recommended for people who have tried other treatment like cortisone-injections, accupuncture etc with little or no success. Electroacupuncture and standard acupuncture are used in the treatment of plantar fasciitis and other foot problems such as neuromas and nerve impingement, numbness in the toes etc. In some cases there is nerve entrapment within the foot combined with referred pain from other areas of the body. Some research suggests that acunpuncture can be effective in the treatment of heel pain. A trigger point is an irritable knot in the muscle tissue. When pressed trigger points are very tender and can cause pain in that specific spot or elsewhere in the body (referred pain). The response to pushing into the knot is a muscle twitch. The foot contains 126 muscles, tendons and ligaments, so there are plenty of ‘hiding places’ for trigger points. Trigger points in the calf muscles often refer pain directly to the bottom of the foot. Trigger point therapy of the lower leg and foot can therefore be successful in the treatment of plantar fasciitis.

Surgical Treatment
If treatment hasn’t worked and you still have painful symptoms after a year, your GP may refer you to either an orthopaedic surgeon, a surgeon who specialises in surgery that involves bones, muscles and joints, a podiatric surgeon, a podiatrist who specialises in foot surgery. Surgery is sometimes recommended for professional athletes and other sportspeople whose heel pain is adversely affecting their career. Plantar release surgery. Plantar release surgery is the most widely used type of surgery for heel pain. The surgeon will cut the fascia to release it from your heel bone and reduce the tension in your plantar fascia. This should reduce any inflammation and relieve your painful symptoms. Surgery can be performed either as, open surgery, where the section of the plantar fascia is released by making a cut into your heel, endoscopic or minimal incision surgery – where a smaller incision is made and special instruments are inserted through the incision to gain access to the plantar fascia. Endoscopic or minimal incision surgery has a quicker recovery time, so you will be able to walk normally much sooner (almost immediately), compared with two to three weeks for open surgery. A disadvantage of endoscopic surgery is that it requires both a specially trained surgical team and specialised equipment, so you may have to wait longer for treatment than if you were to choose open surgery. Endoscopic surgery also carries a higher risk of damaging nearby nerves, which could result in symptoms such as numbness, tingling or some loss of movement in your foot. As with all surgery, plantar release carries the risk of causing complications such as infection, nerve damage and a worsening of your symptoms after surgery (although this is rare). You should discuss the advantages and disadvantages of both techniques with your surgical team. Extracorporeal shockwave therapy (EST) is a fairly new type of non-invasive treatment. Non-invasive means it does not involve making cuts into your body. EST involves using a device to deliver high-energy soundwaves into your heel. The soundwaves can sometimes cause pain, so a local anaesthetic may be used to numb your heel. It is claimed that EST works in two ways. It is thought to, have a “numbing” effect on the nerves that transmit pain signals to your brain, help stimulate and speed up the healing process. However, these claims have not yet been definitively proven. The National Institute for Health and Care Excellence (NICE) has issued guidance about the use of EST for treating plantar fasciitis. NICE states there are no concerns over the safety of EST, but there are uncertainties about how effective the procedure is for treating heel pain. Some studies have reported that EST is more effective than surgery and other non-surgical treatments, while other studies found the procedure to be no better than a placebo (sham treatment).
Stretching Exercises
Exercises designed to stretch both your calf muscles and your plantar fascia (the band of tissue that runs under the sole of your foot) should help relieve pain and improve flexibility in the affected foot. A number of stretching exercises are described below. It’s usually recommended that you do the exercises on both legs, even if only one of your heels is affected by pain. This will improve your balance and stability, and help relieve heel pain. Towel stretches. Keep a long towel beside your bed. Before you get out of bed in the morning, loop the towel around your foot and use it to pull your toes towards your body, while keeping your knee straight. Repeat three times on each foot. Wall stretches. Place both hands on a wall at shoulder height, with one of your feet in front of the other. The front foot should be about 30cm (12 inches) away from the wall. With your front knee bent and your back leg straight, lean towards the wall until you feel a tightening in the calf muscles of your back leg. Then relax. Repeat this exercise 10 times before switching legs and repeating the cycle. You should practise wall stretches twice a day. Stair stretches. Stand on a step of your stairs facing upstairs, using your banister for support. Your feet should be slightly apart, with your heels hanging off the back of the step. Lower your heels until you feel a tightening in your calves. Hold this position for about 40 seconds, before raising your heels back to the starting position. Repeat this procedure six times, at least twice a day. Chair stretches. Sit on a chair, with your knees bent at right angles. Turn your feet sideways so your heels are touching and your toes are pointing in opposite directions. Lift the toes of the affected foot upwards, while keeping the heel firmly on the floor. You should feel your calf muscles and Achilles tendon (the band of tissue that connects your heel bone to your calf muscle) tighten. Hold this position for several seconds and then relax. Repeat this procedure 10 times, five to six times a day. Dynamic stretches. While seated, roll the arch of your foot (the curved bottom part of the foot between your toes and heel) over a round object, such as a rolling pin, tennis ball or drinks can. Some people find that using a chilled can from their fridge has the added benefit of helping to relieve pain. Move your foot and ankle in all directions over the object for several minutes. Repeat the exercise twice a day.
 Overview
Overview Symptoms
Symptoms





 Achilles Tendinitis is the inflammation of the Achilles Tendon located in the heel, and is typically caused by overuse of the affected limb. Most often, it occurs in athletes who are not training with the proper techniques and/or equipment. When the Achilles Tendon is injured, blood vessels and nerve fibers from surrounding areas migrate into the tendon, and the nerve fibers may be responsible for the discomfort. Healing is often slow in this area due to the comparably low amount of cellular activity and blood flowing through the area.
Achilles Tendinitis is the inflammation of the Achilles Tendon located in the heel, and is typically caused by overuse of the affected limb. Most often, it occurs in athletes who are not training with the proper techniques and/or equipment. When the Achilles Tendon is injured, blood vessels and nerve fibers from surrounding areas migrate into the tendon, and the nerve fibers may be responsible for the discomfort. Healing is often slow in this area due to the comparably low amount of cellular activity and blood flowing through the area.




